
In a major step forward for virtual colonoscopy, a Wisconsin HMO has become what is probably the first private insurer in the U.S. to reimburse screening VC for its members who are 50 and older.
Since April the Physicians Plus Insurance Corporation (PPIC) has been paying for VC as well as same-day conventional colonoscopy follow-up when needed. The Madison-based HMO has about 95,000 members in south central Wisconsin.
More than just a boost for the virtual exam, the insurer's new policy amounts to a wager that VC will improve colorectal cancer screening compliance and reduce healthcare costs down the road, while keeping the company competitive in the eyes of its clients.
Dr. Gary Johnson, medical director of Physicians Plus Insurance Corporation, said the new program is not only the right thing to do, it dovetails with one of the group's business goals of improving colorectal cancer outcomes.
"Obviously one of the ways to (improve outcomes) is to make sure that all the appropriate people...get some form of screening," Johnson told AuntMinnie.com. "Unlike some things like breast cancer and cervical cancer and prostate cancer, unfortunately the screening rates of our population for colorectal cancer are not nearly as high as the screening rates for these other cancers, and we get members with advanced colon cancer.... With this new technology we're hoping that more people will elect to get screened, because conventional colonoscopy is not something that a lot of people look forward to."Moreover, the waiting list for conventional colonoscopy at the Madison facility has been as long as a year, and VC is seen as an effective way of trimming the backlog of cases, he said. The university's medical review board approved virtual colonoscopy for colorectal cancer screening, and "that was good enough for us," Johnson said.
"Once one (insurer) covers, the others are left with vulnerability," said Dr. Perry Pickhardt from the University of Wisconsin Medical School in Madison, who is leading the new screening program. "Every year there's an open season where people can switch plans, and I think people might view (VC) as something that's a good thing to offer, and they might switch their coverage."
There was more good news last week when two additional Wisconsin HMOs agreed to add screening virtual colonoscopy to their covered services, he said.
Pickhardt told AuntMinnie.com that he has performed screening virtual colonoscopy on about 40 subjects at the University of Wisconsin Hospital and Clinic in Madison since the program began. Of these, about half have been physician referrals and the other half diagnostic VC cases that were referred from the gastroenterology department following colonoscopy. (Most of the gastroenterology-referred cases were incomplete colonoscopies, but a few patients had comorbidities that made them unsuitable for the sedation that accompanies the conventional exam.) The patient ratio is expected to shift heavily in favor of physician-referred screening now that the testing phase has been completed and marketing can begin, Pickhardt added.
Pickhardt was a principal investigator in the trial that yielded virtual colonoscopy's best performance to date. His group's multicenter Department of Defense study examined 1,233 asymptomatic patients at low risk for colorectal polyps and cancer. VC's sensitivity was 88.7% for polyps 6 mm and larger, 93.9% for polyps 8 mm and larger, and 93.8% for lesions 10 mm and larger, while conventional colonoscopy's sensitivity was slightly lower at 92.3%, 91.5% and 87.5%, respectively (New England Journal of Medicine, December 4, 2003, Vol. 349:23, pp. 2191-2200).
In Wisconsin the patients haven't exactly been knocking down the doors, but then again, they wouldn't have known where to knock until approval to market the program was finally granted last week. Now, Pickhardt said, he can begin to tell local physicians about it, and work on getting screening referrals.
Family practice
The first few days of the program passed with plenty of empty appointment slots, and since Pickhardt couldn't market the program officially, he looked to his family for eligible cases. He even landed a few referrals from his brother, a family practice physician.
"It turns out my parents and my in-laws all have that certain insurance," Pickhardt said last week. "My dad was the very first guy to be reimbursed for screening -- as far as I know the first in the country -- and he had a big 5-cm mass, and as we speak he's in the OR getting it removed. It's probably going to be benign and definitely curable, but I think we saved his life, basically."
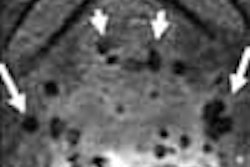
His father's surgery went smoothly, Pickhardt told AuntMinnie.com the next day. And the patient, an otherwise-healthy 65-year-old, was kind enough to allow images of the 5-cm lobulated rectal "carpet" lesion to be included in this article.
 |
| In an asymptomatic 65-year-old male patient, 3D endoluminal view in virtual colonoscopy shows lobulated "carpet" lesion in rectum (arrowheads, above). The top arrow indicates the rectal catheter. Same-day conventional colonoscopy shows the endoscopic view of the same lesion (below). Same-day endorectal ultrasound (as part of conventional colonoscopy) shows a broad superficial lesion along the rectal wall with no evidence of bowel-wall invasion (bottom). The biopsy showed villous adenoma with high-grade dysplasia; histological results are pending. All images courtesy of Dr. Perry Pickhardt. |
 |
 |
Virtually the same protocol
Pickhardt said his exam technique has changed little from the days of the NEJM study. He is tracking all of the new data for research purposes.
Patients receive a double-dose phospho-soda prep the day before the exam, or, if a saline prep is contraindicated, two doses of magnesium citrate. The practice is moving toward a single laxative dose, Pickhardt said.
After cleansing and manual room-air insufflation, the patients undergo multidetector-row CT imaging on either an 8- or 16-detector scanner (LightSpeed or LightSpeed Ultra, GE Healthcare, Waukesha, WI), using 8 x 1.25 mm or 16 x 1.25 mm collimation, respectively, 100 kVp, and 50-100 mAs depending on patient size.
The images are reconstructed at 1-mm intervals for a 25% overlap, and reviewed on a V3D workstation (Viatronix, Stony Brook, NY) using primary 3D interpretation and 2D problem-solving in every case.
Billing and coding
The practice receives $1,600 from the payor for each screening (and diagnostic) virtual colonoscopy. This compares to about $3,000 for a complete optical colonoscopy patient encounter at the academic facility, a figure that includes nursing and sedation recovery time needed for the conventional exam, Pickhardt said.
"Our cost-effectiveness analysis shows that if virtual colonoscopy costs about half of your optical (colonoscopy) charges, (VC) is definitely cost-effective, and even the dominant strategy," he said.
For now, the exams are coded as diagnostic CT colonography with 3D reconstruction, but in July the group will begin using the new Category III CPT codes: 0066T for screening virtual colonoscopy, and 0067T for diagnostic virtual colonoscopy, Pickhardt said.
The names of the two additional HMOs that signed on last week will also be announced once he has done some work for them, Pickhardt said. Both new payors stipulated that the practice use the Viatronix V3D Colon workstation exclusively because it is FDA-cleared specifically for screening CT colonography, Pickhardt said.
Follow-up
The group provides surveillance services for cases that are positive but do not require immediate polypectomy, and the follow-up interval varies with the size of the finding in virtual colonoscopy:
- 8-9 mm polyps are followed up at one year.
- 6-7 mm polyps are followed up at two years.
- 5-mm polyps are followed up at three years.
- 5 mm and smaller polyps are followed up at five years.
- 10 mm and larger polyps are recommended for same-day colonoscopy and polypectomy.
"For anyone with a polyp 6 mm or (larger) we are at least offering colonoscopy," he said. "So far no one has chosen to go on (to colonoscopy) for a 6-9-mm polyp, but we have had two patients go on to same-day colonoscopy." The first was his father, and the second was an asymptomatic man with a single 1.5-cm tubulovillous adenoma. Patients have ranged in age from 50 to 79 years, with most screening subjects in their 50s.
"The time has come, we've tested the system, everything works, and we now have to advertise among our physicians that it's available," Pickhardt said.
By Eric BarnesAuntMinnie.com staff writer
June 4, 2004
Related Reading
CPT codes and the politics of virtual colonoscopy, April 30, 2004
Viatronix gets OK for virtual colonoscopy unit, April 26, 2004
Group credits 3-D reading for best-ever VC results, October 15, 2004
Copyright © 2004 AuntMinnie.com













![Images show the pectoralis muscles of a healthy male individual who never smoked (age, 66 years; height, 178 cm; body mass index [BMI, calculated as weight in kilograms divided by height in meters squared], 28.4; number of cigarette pack-years, 0; forced expiratory volume in 1 second [FEV1], 97.6% predicted; FEV1: forced vital capacity [FVC] ratio, 0.71; pectoralis muscle area [PMA], 59.4 cm2; pectoralis muscle volume [PMV], 764 cm3) and a male individual with a smoking history and chronic obstructive pulmonary disorder (COPD) (age, 66 years; height, 178 cm; BMI, 27.5; number of cigarette pack-years, 43.2, FEV1, 48% predicted; FEV1:FVC, 0.56; PMA, 35 cm2; PMV, 480.8 cm3) from the Canadian Cohort Obstructive Lung Disease (i.e., CanCOLD) study. The CT image is shown in the axial plane. The PMV is automatically extracted using the developed deep learning model and overlayed onto the lungs for visual clarity.](https://img.auntminnie.com/mindful/smg/workspaces/default/uploads/2026/03/genkin.25LqljVF0y.jpg?auto=format%2Ccompress&crop=focalpoint&dpr=2&fit=crop&h=167&q=70&w=250)


